Cardiologist to the Court

Andrejs Ērglis, one of Latvia’s most famous doctors, is from a well known medical family and combines professional talent with personal charm. In his own words, he has raised Latvian interventional heart surgery to a world level. But how can a poor country with one of Europe’s lowest healthcare budgets also be among the world leaders in expensive heart operations using stents, the microscopic structures used to repair damaged arteries? And why, even though it spends so much on such procedures, does Latvia not also lead in reducing the number of premature deaths, with heart disease still the country’s main killer?
I received the following letter one grey afternoon in February from Latvia’s most famous cardiologist, Professor Andrejs Ērglis. “Given your incredible interest in the price of stents, salaries and in me personally, I would like to know whether your report is being done on the orders of any political, economic or individual interest?”
Ērglis, 49, was reacting to my research of six months on why Latvia has for years liberally financed expensive heart operations, when at the same time heart health indicators remain poor. I have read 20 years of articles about Ērglis and interventional cardiology, done a three hour interview with the professor himself, talked with other experts and asked for information from the health services of the Baltic states and hospitals. But there is still no clear answer to the key question – how much do the stents, used by Stradiņš Hospital to open up arteries in patients with heart problems, actually cost?
Stents are used in arteries that have become clogged up. Interventional cardiology has developed rapidly in the last few decades, meaning that heart attacks and premature death can be prevented. The procedure, which takes about an hour, involves making a small incision in the patient’s leg or arm, through which a catheter is passed. That goes up to the affected area, where a small balloon is inserted into the narrowed artery. A stent is then introduced and it keeps the artery open, so blood can flow to the heart.
In the United States, using stents to widen arteries has been recognised as one of the five most overused medical procedures. Due to pressure from manufacturers, expensive stents are used in cases when drugs would have been more appropriate. In 2011, research in the Journal of the American Medical Association showed that the use of stents had been inappropriate in 12 percent of non-emergency cases.
Latvia has become a world leader in the use of stents. Re:Baltica’s calculations, based on 2011 data, show that it carried out 310 stent operations per 100,000 inhabitants.
Among the rich nations of the Organisation for Economic Cooperation and Development (OECD), which Latvia hopes to join, Latvia is second only to Germany in the use of stents. In contrast, neighbouring Estonia carried out 210 operations and Lithuania only 187.
Financing for interventional cardiology in Latvia has also been generous, in contrast to other areas of healthcare. The state gives 24.5 million euros a year on average to the speciality, the most in the Baltic region. Thanks to Ērglis’s enthusiasm and ability to make friends among politicians, cardiologists also make six times more than surgeons working in the main children’s hospital in Riga. Six years ago, speaking to health magazine “36.6”, Ērglis was able to boast: “We have one of the best interventional cardiology laboratories in the world.”
The wide use of stents can be explained by high levels of heart disease, which is the main killer in Latvia and the rest of Europe. However, despite generous financing for cardiology, Latvia has three times the European Union average of people dying prematurely from heart disease, much higher than in Estonia, which uses far fewer stents, and slightly lower than Lithuania.

One key problem is that though Latvia spends millions of euros to treat ill people, not much is devoted to preventive care to stop people ending up in the operating theatre. In 2012 Latvia spent 73 million euros on cardiology, while all health promotion activities got just 90,000 euros.
The government’s priorities in distributing funds were also shown last year when a plan to improve heart health was approved for the period up to 2015. That gave the already generous cardiology budget a further 7 million euros. Even though the plan stated that effective preventive care can cut the death rate by as much as half, most of the money, 78 percent, was set aside for medical procedures. Preventive medicine got just 2 percent, or 118,000 euros.
Though the plan was formally presented by the Health Ministry, it was drawn up by Ērglis and his colleagues. He was also present at the government meeting which considered the plan, ready to answer any questions. There were none.
A few months earlier, Ērglis and Health Minister Ingrīda Circene, who represents the main ruling coalition party Unity, had taken part in a public exercise session with members of the government, measuring blood pressure and urging people to look after their health. Such campaigns come easily to Ērglis, a man of charm who since his childhood has been used to the society of famous and influential people.
Talented Ērglis
Ērglis spent his childhood in the quiet Riga suburb of Āgenskalns, in the house of his grandfather Pauls Stradiņš, the founder of Latvia’s healthcare system, and in the clinic which was to bear the name of the great medical man, just across the street. That is now Erglis’s workplace and the second biggest hospital in Latvia.
Ērglis in his youth dreamt of being a film actor and worked on the radio in secondary school. He finished school with excellent grades and, under the influence of his cousin’s husband, cardiologist Uldis Kalniņš, began studying medicine. Ērglis soon began to work at Kalniņš’s Cardiology Centre and at the age of 26, on April 4, 1990, carried out his first angioplasty to widen arteries. The technique had only been invented 13 years earlier by Swiss doctor Andreas Gruentzig. Ērglis had to read about how to carry out the procedure in specialist literature because there was no way at that time to observe and train in real life.
Conditions in those days in the operating theatre were tough, with angioplasty equipment that was 25 years old. For Andris Saltups, an Australian-Latvian interventional cardiologist, who was in Riga in 1993 for a world congress of Latvian doctors, the conditions in which about 100 angioplasty procedures had been carried out were a shock.
Ērglis and his colleagues invited Saltups to take part in an operation and the words of the head nurse at the time stuck in his head, as she warned that there were only two pairs of sterile gloves for the whole day’s work.
A year later, helped by Saltups and Latvians in the Australian city of Melbourne, Ērglis spent three months training in Australia. On his return, he found it difficult to get used to the poor conditions and began to have problems with alcohol.
“It is not normal that a 25-year-old lad has responsibility for all interventional cardiology. No one remembers this now, but we got no money for this programme for 7 years,” Ērglis told the Ievas Veselība health magazine in 2011.
“Everything we had came from abroad, from here and there. Having to tackle such difficulties at that age … It’s obvious that drink is the quickest way to relax,” Ērglis said, talking openly about his problems.
“We often got phone calls in the middle of the night, I encouraged him not to lose hope and to fight on, telling him that things would get better,” said Saltups. Ērglis did not give up and when Saltups met his young colleague at an international conference in Toulouse in France in 1996, Ērglis related happily that Stradiņš Hospital would soon get modern digital angiography set up, just like in Melbourne.
That was also when Latvia for the first time used stents in the widening of arteries. Saltups came to Riga in October, equipped with donated catheters and stents, but by 1999 he was ready to concede that angioplasty in Latvia was already up to American, Japanese and Australian levels. “It was the first time I felt surplus to requirements as a teacher and consultant,” he said.
Ērglis’s career took off over the following decade. He does not drink anymore and in 2003 he got the Order of the Three Stars, a high level state medal for meritorious service. When Kalniņš unexpectedly died in 2004 of a heart attack at the age of 58, Ērglis stepped into his shoes as head of the Cardiology Centre. He also became the leader of the Latvian Interventional Cardiology Development Society and of a regional organisation in the Baltic states. One year later he became the president of the Latvian Cardiology Society. He is also a consultant to the certification committee of the Latvian Association of Doctors, which hands out and, every five years renews cardiology certificates. He literally has a monopoly on the interventional cardiology sector in Latvia. He is respected and all doors are open to him. He takes part in international research projects and appears at conferences. In a survey by “Ir” magazine in 2012 of the top Latvian researchers, where the main criterion was international citations, Ērglis easily came first. He had had 77 publications since 2007 and had been cited in other authors’ works 536 times.
Ērglis also treats the cream of Latvian society, where there is high demand for a good cardiologist for an elite worn out by stress. He can count several health ministers among his patients, as well a culture minister, a well known composer, two presidents and a clutch of members of parliament. When Education Minister Roberts Ķīlis last year had heart problems, his doctor, Ērglis, told the prime time television news show “Panorama” that the patient had had a stent inserted and that he must cut back on his workload.
“It is good to talk with him, have a chat. He has read a lot, knows about art and literature,” said Normunds Beļskis, who in 2005 was adviser to the then health minister, Gundars Berzinš of the People’s Party. Ērglis came at that time and asked for funds to develop interventional cardiology at Stradiņš Hospital. The minister asked him to draw up a Latvia-wide plan and “sent Ērglis packing.” Three months later, the doctor was back. “He was always well prepared, with presentations and research,” said Beļskis.
Ērglis’s determination and charm paid off. It was during the time when Bērziņš was minister that interventional cardiology got major state support. In 2005, the government decided to spend 6.4 million euros over the following three years to buy seven angiography machines for testing arteries. In 2006, the cardiology programme got 25 million euros. The goal was to reduce deaths from heart disease by 30 percent by 2010, though the reduction reached was only 15 percent.
But such generosity has its price and Ērglis’s image suffered when he took part in a boosting campaign for the People’s Party ahead of parliament elections in the middle of 2006. The media was flooded with adverts featuring well known people praising ministers from the party, including Ērglis, who was seen saying that the state of cardiology was “under the banner” of Bērziņš. The adverts caused controversy because they were illegal and aimed at avoiding limits on party political spending ahead of elections.
Before economic crisis struck Latvia in late 2008, which cut off a lot of the funding of the wealthy pre-crisis years, Ērglis dealt with four health ministers, all from the People’s Party.
He showed himself ready to take on very exotic heights with these politicians in order to improve healthcare. He took a first special health group in 2007 to Mount Kilimanjaro in Africa, a year later went to the Himalayas and then the Andes in 2009. The core of the group was former Prime Minister Aigars Kalvītis, former president Guntis Ulmanis, Health Minister Gundars Bērziņš and his adviser, Beļskis. Ērglis worked out a special training programme for each of them before the trip.
Cardiologists Are The Best Paid
Ērglis can afford exotic trips because he is a wealthy doctor and businessman. According to the Lursoft database of corporate information, he is a direct or indirect co-owner of six companies. The biggest is a/s Sistēmu inovācijas, which had turnover in 2012 of more than 700,000 euros and profits of almost 200,000 euros.
His monthly salary is not known. Despite holding several posts, he has never been an employee of the state and is exempt from publicly declaring his income, but conclusions can be drawn from the information that is available, that his salary at Stradiņš Hospital could be about 10,000 to 14,000 euros a month before tax. The State Tax Office last year collated figures at the request of Re:Baltica on the 50 biggest salaries in various job categories at the five biggest state and local authority hospitals, as well as at three private hospitals. The main conclusion was that cardiologists are the best paid doctors in the country.
Anonymous data shows that a doctor named only as “a cardiologist” earned the most last summer, with a salary in May, June and July of between 10,658 euros and 15,221 euros a month. Of the 50 biggest salaries, 14 were those of cardiologists and 6 of surgeons.
The Tax Office did not say which of the cardiologists were interventional cardiology specialists, but checks by the State Audit Office in 2009 at Stradiņš Hospital showed that it was just such specialists who earned the most.
The checks showed showed that one doctor at the Interventional cardiology laboratory earned the most among all doctors at the hospital, bringing in 6,400 euros a month on average. One nurse at this laboratory also lead salaries among more junior staff at almost 2,000 euros. The top salary among all department chiefs was that of the head of the Cardiology Centre, a post occupied by Ērglis, at more than 10,000 euros a month, where 80 percent of the earnings are variable.
“The system works in a perverse way,” said Maris Rēvalds, head of the Healthcare Workers Employer Association. “Everything depends on how well you can lobby. Ērglis does that very well, he puts his heart and his soul into looking after his area, but the price is that people at the other end of the scale are poverty stricken,” he said. While some have standards of living similar to developed countries in Europe, other specialists are leaving Latvia, leading to a lack of neurologists, rheumatologists and endocrinologists, he added.
The Health Ministry promised to carry out a review after the State Audit Office revealed big differences in pay, not only between hospitals, with salaries for equivalent jobs at the Eastern and Children’s Hospital being lower than those at Stradiņš, but also within hospitals. The state secretary at the ministry then, as now, was Rinalds Muciņš. He says that data has been collected, but nothing has changed. The ministry is a controlling shareholder in state hospitals, but Circene told Latvian television’s interview show “1 on 1” that she could not influence doctors’ salaries as they were set by the boards of hospitals.
Muciņš said Stradiņš Hospital justified the big salaries for interventional cardiologists on the grounds that they “bring in most of the hospital’s budget. The cardiology programme is a major contributor to profits.” That statement is backed up by the facts. The state last year paid more than 42 million euros to the hospital for medical services, with the two biggest portions for adult cardiology at 9.2 million euros and the insertion of stents costing 6.6 million euros. The remaining amount is divided between more than 30 other medical services.
The new chairman of the board at Stradiņš, Dins Šmits, who is the former head of GlaxoSmithKline in Latvia, has promised to review the salary system, saying that such differences are not justifiable. At the same time, Šmits and Ērglis know each other well. They both play in tennis competitions and the drug company which Šmits used to represent recently donated more than 33,000 euros to cardiology societies headed by Ērglis. Another new member of the board at Stradiņš, the board chairman of the Children’s Hospital, Anda Čakša, once climbed Japan’s highest mountain with Ērglis. The drug company she used to lead, Sanofi-Aventis, at that time donated almost 35,000 euros to organisations headed by Ērglis.
Ērglis himself rejects any criticism. He told Re:Baltica that his salary was appropriate for what he does. He says cardiologists work intensively and that what he earned at Stradiņš was his main source of income, unlike other specialists, who also work privately. “None of our patients are on the ward in an awkward situation, wondering why no one is coming to operate on them,” he said. He said his base salary was 1,280 euros, with the rest being a variable salary for work on the ward and with foreign patients.
However, work with foreign patients is a small share. Interventional cardiology services were given to 21 foreign patients last year, mostly from CIS countries, which brought in 40,000 euros to the hospital.
“Given that we have a world-class level of interventional cardiology, it would be good to have more foreign patients,” said Māris Taube, head of the National Health Service. “Estonia has well developed eye surgery, Lithuania has cell medicine, but Latvia does not have any strong area which would bring in money.”
One source of income which lacks clarity is clinical trials. According to data from the State Agency of Medicines, there have been 14 clinical trials in Latvia since 2009, with manufacturers testing the efficiency of stents. The data is confidential and the agency does not know who orders the tests and where they take place. Stradiņš Hospital says that it made 97,000 euros last year from interventional cardiology clinical trials, but does not know how much Ērglis gets from that.
Medical expert Uģis Gruntmanis criticises what he sees an absurd system. “It is absolutely impossible to understand how Stradiņš Hospital, which belongs to the state, can let money for clinical trials be transferred privately to doctors. This system lacks transparency and it creates the kind of huge conflicts of interest which should not be allowed in any developed country,” said Gruntmanis, an associate professor at the University of Texas and a special advisor to former Health Minister Juris Bārzdiņš and former Social Affairs Minister Ilze Viņķele.
How Much Does A Stent Cost?
So if foreign patients and clinical trials only bring in relatively small amounts, where does the large profit come from for cardiology work? The answer is – it comes from the state.
Until recently, the National Health Service put no limits on payments for stents, which are used in 90 percent of angioplasty procedures. Such procedures cost the state 24.5 million euros a year, treating 6,200 patients and, compared with other areas, cardiology is one of the biggest expenditure items in the health budget.
Latvia uses two kinds of stents, simple metal ones and more modern and expensive ones which are coated with medicine to stop the artery closing up again. There are dozens of different kind of stents and their prices vary, but the official payment set by the state is 854 euros for a simple stent and 1,700 euros for a medicine-coated stent, known as drug eluting. This is just one part of the angioplasty procedure, which altogether costs the state 3,477 euros for the regular stent and 4,757 for a drug-eluting stent, including materials, the doctor’s work and a stay in hospital.
In 2011, the Health Ministry for the first time set quotas for the more expensive stent. Specialists cited research by Britain’s National Institute for Health and Care Excellence that financial benefits from the use of drug eluting stents only came when the price difference between the two was just 225 euros, whereas in Latvia the difference was four times as much.
The cardiologists staged a revolt and Ērglis told the television news show “Panorama” that some patients, diabetics for instance, could not use the simple stents and that the ministry’s decision would put cardiology back by 20 years. However, no agreement was reached between the ministry and doctors and in 2012 the state paid only for cheaper metal stents. Last year, a compromise was reached and now 10 percent of stents paid for by the state are drug eluting.
The changes hit Stradiņš Hospital most because it gets the most serious heart cases, which usually need the more expensive stents. In 2011, some 1,403 drug eluting stents were inserted and only 694 of the cheaper ones. Ērglis has been angered by such moves and has continued his fight. He last year wrote to the Health Ministry, noting that in 2012 a third generation of stents had been developed which are biodegradable in the body and that the use of metal stents was out of the question.
“People in Latvia deserve medical care which is up to the standards set by guidelines in Europe and other developed countries for the 21st century,” he wrote.
But medical expert Gruntmanis disagrees. “If the health budget has such limited resources as now, then we cannot afford mercedes’s to all cardiology patients while other patients have to receive ladas,” he said. Gruntmanis has already noted, in a 2009 article for news portal Delfi, that Latvia pays a lot more for stents than rich countries in Europe, the United States and Canada.
In fact, the state itself does not know how much stents really cost. The State Audit Office in 2011 said the bodies overseeing health institutions had “no figures on which to base the calculation of tariffs for services.” Stradiņš Hospital is in the same position, including for stents.
“To tell the truth, I’m not sure,” said National Health Service boss Taube when asked about setting tariffs for services. The price of stents has not been looked at since 2008 when centralised buying for all hospitals was introduced. That system was later dropped because doctors said the wrong things were being bought. Taube is clear that he is afraid to ask doctors how much stents cost because there is no basis on which to judge whether the costs are appropriate. The number of experts, at least in the Baltic region, is limited. “They are all Ērglis products. So what we do is that we carry out mechanical cuts (of tariffs),” Taube said.
“We got a bit carried away with the use of stents, compared with our financial resources,” said State Secretary Muciņš. At the same time, he noted: “Maybe it is good that our goal is to be as good as the Germans, but at the level of the state we have to give the same priority to all areas.”
The government is now trying to reduce the cost of expensive stents because this money could be used to treat other illnesses. “Interventional cardiology currently has high prices, but other specialists are getting paid in pennies,” said Taube. For instance, while one stent insertion can cost as much as 4,800 euros, the price for the removal of a breast of a woman with cancer and her stay in hospital is just 690 euros. An operation for a bleeding ulcer and hospital stay is 630 euros, while a liver and gallbladder procedure is 1,390 euros.
Efforts by Re:Baltica to find out the price of a stent in the Baltic states led to a merry dance which lasted several months. Lithuania and Estonia pay hospitals according to the diagnosis related group (DRG) system, which is also used in several EU countries for reimbursing hospitals for medical care, and which this year will be introduced to Latvia.
This means that neighbouring countries do not separately regulate the use of simple or expensive stents, meaning it is difficult directly to compare the cost. So Re:Baltica
calculated the 2012 average cost by dividing the total amount of money spent by the number of patients. Estonia spent the most for treating artery problems at 7,525 euros, Latvia 3,951 euros and Lithuania 1,725 euros. Explaining why the operation costs so much in Estonia, a representative from the local health insurance fund said the rates for state financing had not been reviewed since 2002, when stents were much more expensive. The conclusion from the Lithuanian data appears to be that only cheap stents are being used.
Throughout the Baltic states, it is the hospitals themselves which purchase the stents and the health services of each country have no information on the price. The biggest Estonian hospitals declined to reveal the price of stents, while a spokeswoman for the University Hospital in Vilnius said it was difficult to get information from the cardiologist in charge as he did not want to cause problems for his Latvian colleagues. Finally, it was only Tartu University Hospital in Estonia which replied. It said the average price for a simple stent was 210 euros, and 400 euros for a drug eluting stent.
These prices were much lower than those given by the Stradiņš Hospital, which was nearly 500 euros for a metal stent and about 1,300 for a drug eluting stent. But the methodology used by each hospital is unclear when it comes to calculating the average cost. Latvia’s largest hospital, Eastern Hospital, said the three most commonly used stents cost between 230 and 500 for the metal version.

So it is now clear how cardiology makes a profit for Stradiņš Hospital. If the state has calculated the tariff for simple stents at 900 euros, but the hospital buys them for 200, then the difference can be spent on other things, like salaries and other areas of medicine.
Another particular aspect of the way in which hospitals buy goods is donations which come from pharmaceutical companies for doctors to go on courses abroad and to conferences. For instance, Ērglis has posts in 10 organisations, and the Society for the Development of Interventional Cardiology, which he leads, has received donations worth 840,000 euros since 2008. On the list of donors are the big firms which win cardiological goods’ tenders with the hospital.
Altogether, companies which have donated to Ērglis’s organisations have won tenders worth 40.4 million euros over the last four years. For instance, Arbor Medical donated 85,000 euros and won a contract worth 6.2 million euros, Johnson&Johnson AB donated 72,000 and got an order worth 5.8 million euros while Ilsanta UAB donated 40,000 and has won orders worth 9.7 million euros.
And The Result Is?
“I am bit fed up talking about stents all the time,” says Ērglis when I meet him in October as he rushes into his office. He talks quickly, a bit chaotically. He absolutely rejects the idea that interventional cardiology has a privileged place and jumps up to escort me to the ward to show me his colleagues’ work, something he does with all journalists.
“I get a bit upset at that question because we spend a lot of time on preventive measures,” he answers when asked why such a small amount is spent on avoiding heart disease. He says that in 2001 it was impossible to get the media to write about medical issues. “Look at how much there is now on the Internet,” he added.
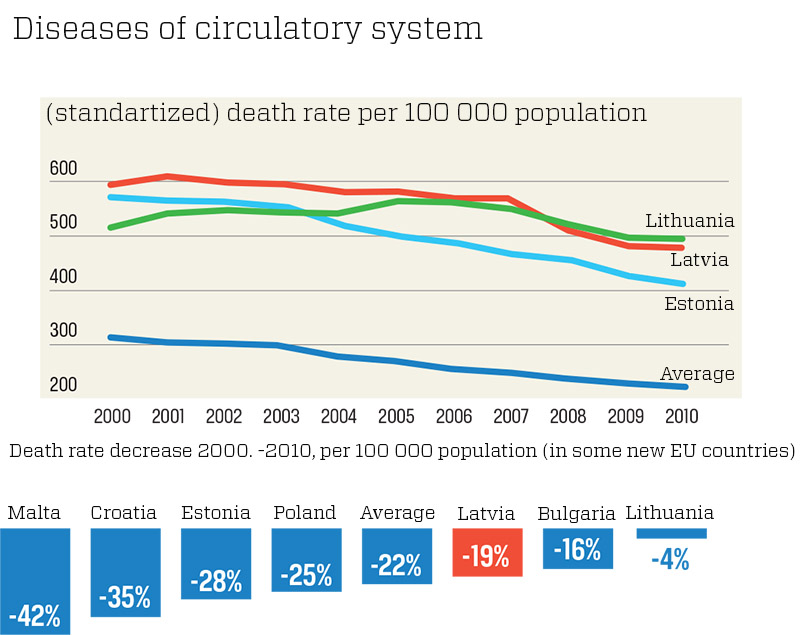
But articles are not enough. Despite the millions of euros spent on cardiology, Latvia still has many premature deaths due to heart and circulatory illness. The number has gone down by 14 percent in the last decade, but in Poland it has fallen by 26 percent and in Estonia by 40 percent. On average, the level has fallen by 25 percent in the new countries of the EU, according to figures from the World Health Organisation (WHO). In absolute numbers, there were 2,606 deaths before the age of 65 in Latvia in 2012 due to heart problems.
Both Estonia and Poland use far fewer stents than Latvia, but have better results. Why is that? Ērglis says the statistics in Latvia are wrong. He says doctors often give heart problems as the reason for death, but if someone freezes to death, then the fact the heart has stopped beating is not the real reason for that person’s demise. A study is currently being carried out to look at the cause of mortality of 1,000 people who died due to cardiological problems and Ērglis said he expected that some 10 percent of these instances would show the cause of death was different than the officially given reason.
Even if this assumption is borne out, then the experience of other countries shows the best way to avoid premature death from heart problems is preventive medicine, an area where Latvia lags far behind. The Polish experience shows that getting rid of risk factors accounted for half of the reduction in mortality rates. Reducing cholesterol produced 39 percent of the reduction, while physical exercise contributed 10 percent. Just 9 percent of the overall impact came from acute coronary care, where stents are used.
Ireland is another good example. It has reduced deaths from heart and circulatory illness by 42 percent. A third of the 211 recommendations it made were connected to improving health, like raising tobacco excise duties above the level of inflation, advice on healthy eating, having an alcohol policy and making physical activity more popular. It also said the links between health organisations and family doctors should be improved, something which is an area of weakness in Latvia.
The priorities in Latvia can be seen in how the money for cardiology is spent. Most of the money, 42 percent, goes to hospitals, with the next biggest category being drugs at 35 percent. Out-patient treatment comes next, but there is not even a separate splitting out of financing for preventive activities. The new plan to reduce heart and circulatory illness does not really improve things as just 2 percent of the extra financing goes to preventive steps like healthy living and an anti-smoking campaign. A further 700,000 euros will come from screening various age groups for heart problems and there is just 4,000 euros for measures to educate family doctors. No money has been set aside for rehabilitation after the insertion of a stent, which is a key factor.
Of course, a lot of money is not the only way to improve health and reduce the cost of care. A few decisions at the level of the state could suffice, but those are hindered by wealthy lobbies. They have stopped efforts to raise taxes on alcoholic drink and cigarettes, in a situation when stopping smoking can in one year reduce the risk of heart disease by half. Food manufacturers also object to limits on salt and trans-fats. Re:Baltica’s research has shown that snacks containing sugar and unhealthy fats are being sold in unlimited quantities in Latvian schools.
There is currently no sign the Health Ministry will beat such powerful lobbies. In the meantime, those working in the health sector struggle to grab the biggest slice possible of a health budget which is among the smallest in the European Union.
In the end, it is the strongest who win. Those like Andrejs Ērglis — a talented cardiologist, who has saved the lives of many and made his country famous throughout the world, but who seems too expensive for Latvia.
INDEPENDENT JOURNALISM NEEDS INDEPENDENT FINANCING
If you like our work, support us!
Thanks to Baiba Zālīte and Rudīte Spakovska for help with data collection and analysis.

